



A disease you’ve never heard of is becoming increasingly common and carries a very poor prognosis.
For me, one of most important aspects of attending the ACR Annual Meeting is to learn about conditions that I don’t know and that may afflict my patients when I return back home. This year’s meeting was no different.
The disease that caught my attention? Systemic juvenile idiopathic arthritis-associated lung disease (SJIA-LD). This newly-described disease was featured in the Pediatrics Year in Review, as well as in several sessions, abstracts, and study groups. Dr. Grant Schulert and his colleagues at Cincinnati Children’s Hospital have led the efforts to better understand this condition. So what did I learn?
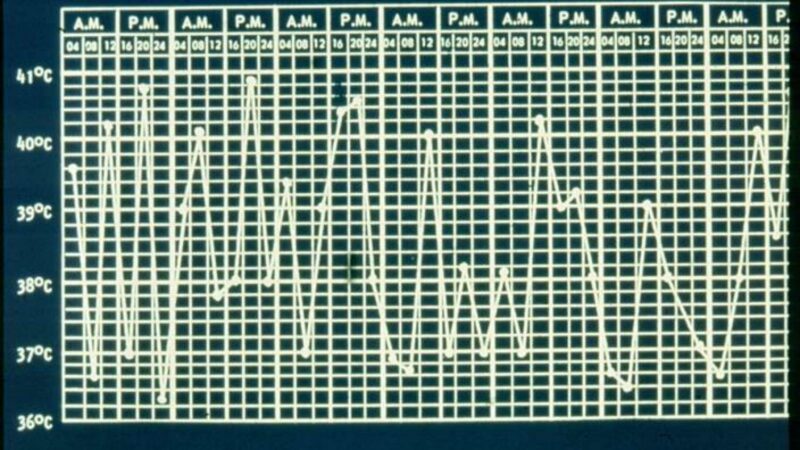
For the adult rheumatologists in the room, SJIA was the original Still’s disease, the pediatric version of what we now call adult onset Still’s disease (SJIA). It is characterized by daily spiking fevers, arthritis, hepatosplenomegaly, lymphadenopathy, and a salmon-colored rash. Up to now, lung disease had not been recognized as a major complication of this condition.
However, Dr. Schulert and others began seeing patients with SJIA who were developing respiratory symptoms unlike those that had been described previously, and they called this condition SJIA-LD.
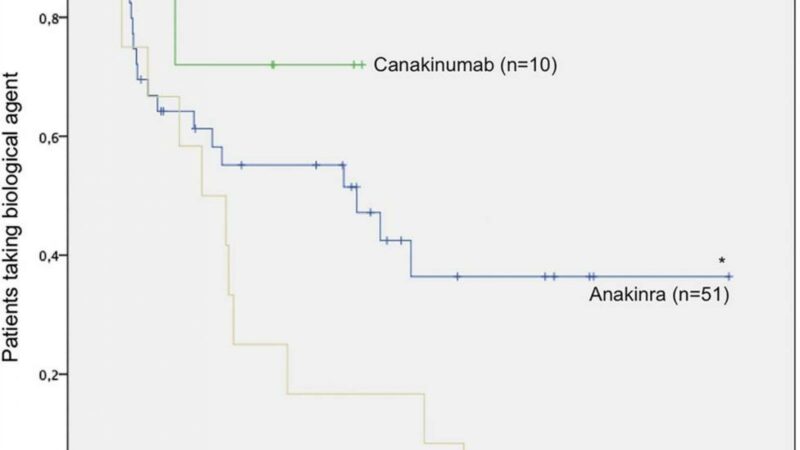
Patients with SJIA-LD typically present with mild dyspnea, a chronic cough, and may even develop clubbing of the fingers. CT imaging findings include pleural, bronchial wall, or peribronchovascular thickening, septal widening, with commonly seen ground glass opacities, lymphadenopathy, and peripheral consolidation. Histopathology reveals lymphoplasmacytic infiltrates and features of pulmonary alveolar proteinosis. Prognosis is poor; studies have shown mortality rates up to 37-68%.
Risk factors for developing SJIA-ILD include an earlier age of SJIA diagnosis, prior episodes of macrophage activation syndrome (MAS), adverse reactions to biologic therapy, and higher serum IL-18 levels.
The cause of SJIA-ILD remains unclear. It is possible that certain genetic factors or environmental factors such as infections may be playing a role.
Better understanding of the cause of SJIA-ILD may help to provide us with guidance on its management. I hope that some answers will become available at #ACR20…stay tuned!

Author: John Swope
Related Content
-
 August 8, 2019
August 8, 2019A single-center cohort analysis shows that lung disease (LD) is increasingly seen in…
-
 May 5, 2015
May 5, 2015A retrospective review of 77 SoJIA patients revealed that 50-70% achieved inactive disease or remission…
-
 March 13, 2019
March 13, 2019First-line treatment of systemic juvenile idiopathic arthritis (JIA) with anakinra (Kineret) was highly…
-
January 17, 2018
Since 2000, the German Biologics register (BiKeR) has prospectively enrolled children with juvenile…
-
 November 9, 2021
November 9, 2021 -
 February 25, 2020
February 25, 2020Rheumatology has a comprehensive overview of methotrexate (MTX) and the risk of lung injury,…